Kate Lines,1 Junior Alves Sebbanja,2 Stanley Dzimadzi,3 Diana Mitlin,4 Patience Mudimu-Matsangaise,5 Vinodkumar Rao6 and Happiness Zidana7
The Covid-19 pandemic’s health impacts on low‑income urban communities have not been insignificant, but the results of state responses and shutdowns implemented without adequate consideration of poverty consequences have been very serious. In this context, vaccination is one way – among many and varied actions needed – in which people can reduce risk of further exclusion. This article summarises early findings from a study focusing on the experiences of communities in informal settlements in four major cities in the global South – Harare, Kampala, Lilongwe, and Mumbai – which was conducted in partnership with national affiliates of Shack/Slum Dwellers International (SDI). By providing a snapshot of how global vaccine inequalities play out at the local level, we aim to contribute to understanding the challenges faced by low‑income residents in informal settlements in accessing Covid-19 vaccines and their perceptions of those challenges, and to generate insights about good practices to help ensure more equitable vaccine distribution.
Informal settlements, Covid-19, access to vaccines, India, Malawi, Uganda, Zimbabwe, pandemic, urban, community insights.
The Covid-19 pandemic has been hugely disruptive, socially and economically, and its impacts experienced unequally and compounded by existing inequities. Established vaccine programmes in wealthier countries mean that for many, a return to normal life is well under way, albeit within a flawed status quo that could be challenged by new variants. However, the prospect of vaccines supporting recovery efforts in low-income countries (LICs) is very different, where on average 14 per cent of populations have been vaccinated – as compared to 58 per cent in lower-middle-income countries (LMICs), 81 per cent in upper‑middle-income countries, and 79 per cent in high-income countries (Our World in Data n.d., as at 9 March 2022).
Lack of access to effective vaccines means a slower recovery for economies. For people, it means the available protection measures against new waves of infection continue to be limited to controls such as curfews, social distancing, closing businesses and markets, and restricting mobility and public transport. Over the course of the pandemic, these measures to restrict human interaction have been particularly devastating to communities living and working in informal settlements in cities and towns in the global South. Livelihoods, education, businesses, relationships, and care responsibilities have all been severely affected, disproportionately so for young people, women, migrants, and informal and self-employed workers (ILO 2021). The new ‘new poor’ – the 150 million people driven into extreme poverty in the past two years – are more likely to live in urban areas and be drawn from the 1 billion people worldwide who live in informal settlements (Sánchez-Páramo 2020).
Drivers of impoverishment affecting informal settlement communities during the pandemic have included lost income and employment, travel restrictions limiting access to markets and earning opportunities, and the rising cost of staples (Lenhardt 2021). First lockdowns in particular brought a huge share of many cities’ economic activity to a halt almost overnight, leaving people suddenly without a way to make a living. For example, in Harare and Nairobi, informal markets on which communities depend for income and food were demolished or closed. An April 2020 survey in Mukuru informal settlement in Nairobi found 90 per cent of households to be food insecure, mostly due to insufficient income and lower availability of food (Shupler et al. 2021). Even the requirement to wear a mask to participate in social or economic activities creates an additional financial burden (Braham and Ogando 2021).
Communities living with insecure land tenure have been especially badly hit. They are more likely to lack basic services such as water and electricity or be forced to pay relatively higher prices for these to informal suppliers, further undermining capacities to manage pandemic pressures (Corburn et al. 2021). It is harder for authorities to establish impacts and plan responses in undocumented areas, and communities with perceived illegal residence may not be factored into formal relief efforts or qualify for social safety nets (Cities Alliance 2021). Eviction – either because households can no longer afford to pay rent or through demolitions – worsens Covid-19 transmission risks when households resort to sharing cramped spaces with friends and relatives, or migrants return to rural homes (Dupraz‑Dobias 2020).
When Covid-19 vaccines are available, the World Health Organization (WHO) advises countries to ensure priority access for groups at risk of experiencing greater burdens from the pandemic (WHO 2020), including homeless people and those living in informal settlements. However, this latter group is so large that it makes prioritisation difficult. In terms of health burdens, vaccination can help protect communities living and working in high-risk conditions: at high densities in underserviced areas lacking or sharing basic services such as water and sanitation. In terms of socioeconomic burdens, vaccination allows people to safely participate in their own and their community’s economic recovery – by returning to jobs, trading again in markets, and travelling to work and school on public transport.
The pandemic’s health impacts on low-income urban communities have not been insignificant, but the results of state responses and shutdowns, implemented without adequate consideration of poverty consequences, have been very serious. Governments urgently need to assess and address the effects of infection control measures – both already taken and likely needed in future – and in this context vaccination is one way in which people can reduce risk of exclusion.
The purpose of this article is to contribute to understanding the challenges faced by low-income residents in informal settlements in accessing Covid-19 vaccines, and their perceptions of those challenges. It provides a snapshot of how global vaccine inequalities play out at the local level, with specific focus on the experiences of residents of informal settlements in four major cities in the global South. The article summarises the context, methodology, and early results of a three-month survey of community leaders living in 22 informal settlements in Harare, Kampala, Lilongwe, and Mumbai. By uncovering real-time trends around vaccination rollout within informal settlements of particularly vulnerable cities, the project aims to generate evidence and insights about good practices which can help ensure more equitable vaccine distribution. In each city, the research is conducted in partnership with national affiliates of the global network Shack/Slum Dwellers International (SDI).
In the next section (Section 2), we discuss the broader context for the study, with a focus on the dynamics of Covid-19 vaccine inequity observed at global and in-country levels. Section 3 outlines the study methodology. In Section 4, we focus on each city in turn to summarise early findings, drawing on initial survey data. Section 5 concludes.
Vaccine access has become the principal fault line along which the global recovery splits into two blocs, those that can look forward to further normalization of activity later this year (almost all advanced economies) and those that will still face resurgent infections and rising Covid-19 death tolls. The recovery, however, is not assured even in countries where infections are currently very low so long as the virus circulates elsewhere.
(IMF 2021)
The scandal and short-sightedness of global Covid-19 vaccine distribution to LICs is well documented and vaccine nationalism continues to exacerbate global inequities. By buying up future stocks, rich countries outcompete others and undermine global solidarity efforts such as Covid-19 Vaccines Global Access (COVAX), the programme that they are financing to deliver doses to poorer countries (Horner 2021). India’s mid-2021 decision to halt vaccine exports was a further setback, cutting COVAX’s access to the Indian manufacturers on which it was overly reliant. The African Union’s African Vaccine Delivery Alliance also had limited success (Jerving 2021).
Resultant costs to LICs are high, in relative and absolute terms. Covering the costs of vaccinating 70 per cent of the population requires LICs to increase their health-care spending by 57 per cent on average; for wealthy countries this figure is 0.8 per cent (UNDP n.d.). Delayed vaccine timelines expose populations to greater risks from new waves or variants and mean lost economic growth from a delayed recovery as well as less easily quantifiable missed economic opportunities such as the effects of protracted lockdowns on schooling.
In late 2021, when our study took place, Covid-19 vaccine supply to LICs through COVAX appeared to be slowly ramping up, as wealthy countries began donating more doses, India relaxed its export ban, and efforts had begun to be made to tackle underlying issues such as patent restrictions and the need to diversify vaccine manufacture by bringing more low- and middle-income countries into the supply chain (Schiffling 2021). A few months later, as this article was finalised, the picture of global recovery was changing more rapidly. The emergence of the Omicron variant has made it apparent that vaccines do not prevent Covid-19 infection per se, leaving vulnerable people exposed. Despite such constraints, the global North continues to open up, in an uneasy status quo where the potential for things to close down again is in part linked to the possibility of new variants – which are most likely to emerge in contexts of still-high rates of infection and low rates of vaccination.
This should present an even stronger logic for prioritising vaccination in LICs and LMICs, but it remains to be seen whether these even clearer links between North and South in the context of Covid-19 will translate to a recognition that success in the North depends on social justice in the South, or if the context will continue to be a failure to act, on self-interest grounds.
Meanwhile, most African and some Asian countries will still not achieve widespread vaccine coverage until well into 2023 (Economist Intelligence Unit 2021). The need is therefore even more pressing for local and national governments to work to understand the impact of the Covid-19 virus on vulnerable groups, support organised community efforts to build or recover lost resilience, and to put evidence-based policies in place to mitigate the effects of likely future control measures.
Where lives and livelihoods have been disproportionately affected by pandemic control measures, and pre-existing physical or socioeconomic factors compromise capacities to recoup losses or weather further shocks, prioritising vulnerable groups in Covid-19 vaccine rollout becomes an economic and social justice issue. And when global vaccine supply issues continue to limit national progress, policy that prioritises these groups for vaccination can therefore help them to recover faster, mitigate further exclusion, and become more resilient to future lockdowns.
Mandates or restrictions based on vaccination status can encourage uptake but exacerbate inequalities, especially where supply or distribution is an issue. In the context of the Covid-19 virus, these are likely to draw on existing policy approaches around established vaccines, require compulsory vaccination for groups such as health workers, or restrict unvaccinated people’s access to public spaces or activities. In some contexts, private companies are also requiring their employees to be vaccinated. Monitoring the effects of measures to encourage uptake could help avoid disproportionately penalising already hard-hit and vulnerable groups.
Governments must also tackle local-level inequalities in vaccine accessibility – for example, where vaccine clinics are located and their opening hours, and how and what information is disseminated. Informal or casual workers, and self-employed people in particular, face both direct costs and lost earnings in travelling to vaccine centres or waiting in long queues. And studies of Covid-19 vaccine uptake have found a strong nexus between information gaps and the digital divide among marginalised groups, who are less likely to have access to the technology needed to book vaccine appointments or get reliable information about availability, venues, and side effects (Badiuzzaman and Akter 2021).
Globally, Covid-19 vaccine development has been characterised by unavoidable medical uncertainty, governments interpreting health risks differently in different country contexts, and widespread public misinformation. This means that public hesitancy also exists in LICs and LMICs, as it does in richer ones – although in most cases supply and distribution still appear the bigger challenges. Influencing factors on hesitancy vary between and within contexts and cultures. Surveys in Togo and Bangladesh found low trust in government to be a major reason for Covid vaccine hesitancy (Brackstone et al. 2021; Badiuzzaman and Akter 2021). A perception study across 15 African countries found widespread concerns about the safety of Covid-19 vaccines as compared to established vaccines, with scepticism highest in young people, women, urban dwellers, and unemployed people (Africa CDC 2021). Misinformation and disinformation are widespread: half of respondents in the Africa CDC study believed Covid-19 to be a ‘planned event by foreign actors’ (ibid.: 5). However, these findings are very different from early discussions with SDI federation leaders from Ethiopia, India, Kenya, South Africa, and Zimbabwe about vaccine perceptions, which concluded that communities were more concerned about potential costs and securing access to vaccines than with threats to uptake from hesitancy and scepticism (Mitlin et al. 2020).
Survey cities were selected in consultation with SDI’s secretariat because (1) they represented a diversity, (2) the country affiliates (or ‘partner organisations’) were keen to take part and considered the study to be particularly relevant in their context, and (3) we had the opportunity of going directly to trusted community leaders who were familiar with the research process. In addition, all countries had begun to roll out Covid-19 vaccination.
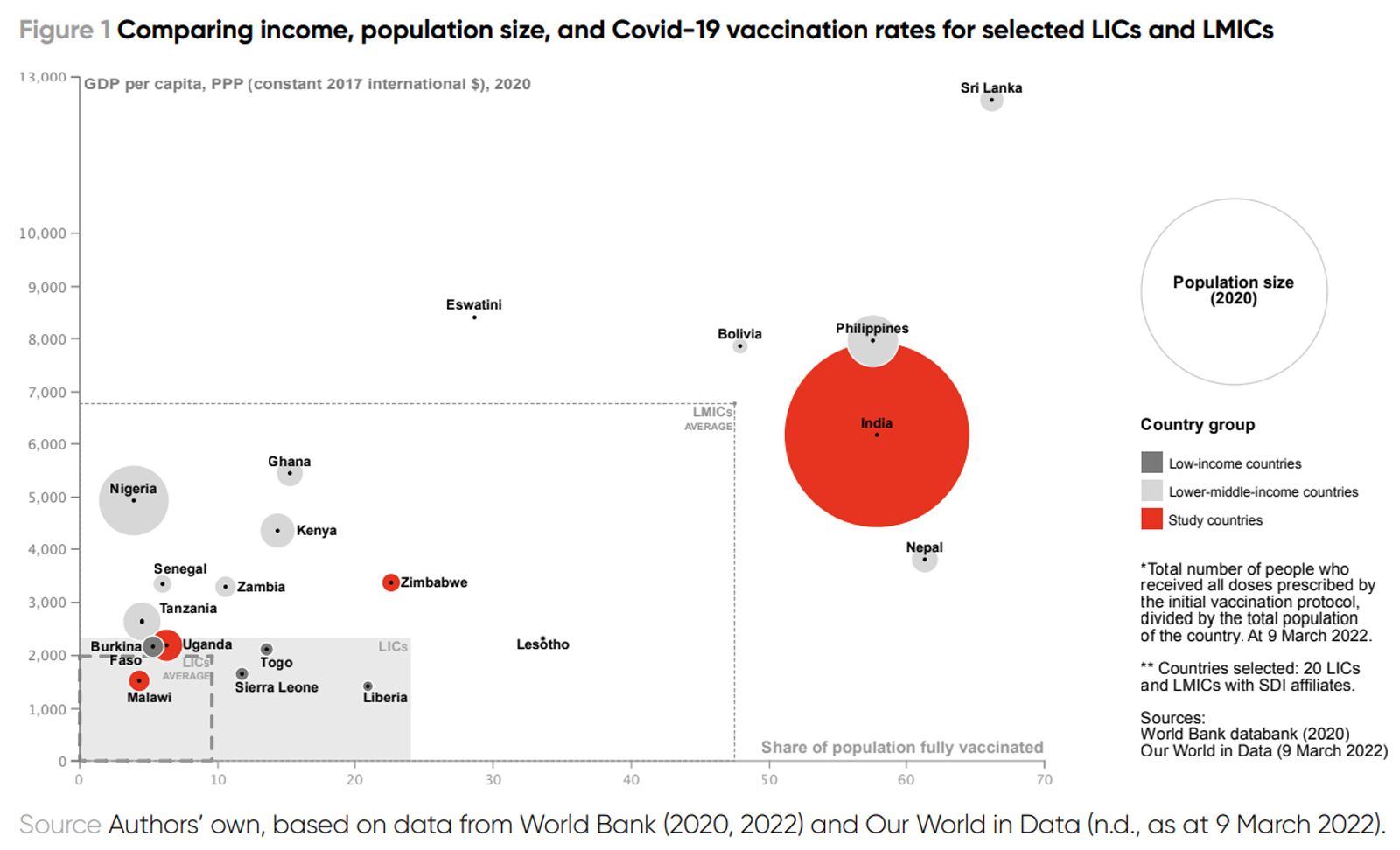
The study was designed as a pilot which, if valuable, could be extended to other cities or over a longer time frame. The picture may well differ in low-income communities in other countries or regions depending on many considerations, not least the national vaccination rate, itself a factor of a country’s access to vaccines and its local distributional capacities. Figure 1 compares the four study countries’ vaccination rates with selected others.
Note: Click to view a larger version of this image.
The phase of research described in this article was conducted concurrently in each city over a period of three months, August–November 2021, with data collected fortnightly (i.e. six iterations in total) using a semi-structured questionnaire. In the fast-changing context of Covid-19 vaccine supply and rollout, we considered that there was a potential for tracking change every two weeks – for example, in vaccination levels or availability at venues – but that more frequently would not be cost-effective.
Each of the four SDI affiliates selected five to six informal settlements in their city to be study areas. The 21 settlements selected represent a geographic spread within each city and a context-specific range of settlement types. In each, there is a strong SDI federation presence or relationship with the neighbourhood. Partner organisations, supported by federation leaders, then recruited around 15 survey respondents from each settlement (i.e. 75 in each city and 300 across the entire study). Respondents were interviewed individually by local professionals or community-based data collection experts.
Our survey sample was not selected at random, and we do not seek statistical validity with this sample size. Rather, the objective was to support SDI affiliates in tracking the situation in several settlements, for which they identified a range of trusted community leaders who could be expected to have a good sense of what is going on in their communities. We defined ‘community leader’ broadly and in each settlement sought to speak to a diversity of traditional leaders, youth leaders, community health‑care workers, religious leaders, and SDI federation leaders, among other groups, both male and female and across a range of ages. Choice of sample size also relates to affiliates’ earlier experiences of dropout due to the scale of pandemic-related disruption.
A draft questionnaire was circulated for comment within partner organisations and to federation leaders, the feedback process ensuring that phrasing and terminology were locally appropriate and that data collection objectives aligned with affiliates’ own objectives. The Mumbai team translated the questionnaire into Marathi; all others were in English. Before launch, the survey and participant consent processes were tested by a handful of community leaders in each city, who provided valuable feedback that led to some adjustments.
We used open and closed questions to capture both qualitative and quantitative information. Respondents were asked some questions about themselves and some about their community. The survey was designed such that if necessitated by Covid-19 restrictions, interviews could be carried out by phone, but in the end it was possible to conduct most interviews face-to-face. Data entry was online using the Qualtrics platform.
During the period of data collection, we also compiled local research teams’ observations about changes and developments in their local vaccine rollout efforts, in order to place the survey data in a wider setting. However, with limited project resources, we rely for further context on other studies and documentation, including other Covid Collective research.
In this section, we focus in on each city in turn to summarise early findings by drawing on data from our first two surveys, run concurrently in each of the 21 settlements in late August and again in mid-September 2021. We present the discussions below as a snapshot of what was happening in each location at this time. To give context to the survey data analysis, accompanying external figures date from roughly the same time period.
As our third survey began, Zimbabwe was among only 15 African countries to meet the WHO target to fully vaccinate 10 per cent of the population by October 2021,8 with 20 per cent of the population (3.1 million) vaccinated at least once and 15 per cent (2.3 million) fully vaccinated (Our World in Data n.d., as at 30 September 2021). Official national cumulative Covid-19 figures for the same period were 130,500 reported cases (8,600 per million population) and 4,600 deaths, with excess deaths estimated at 16,000–41,000 (The Economist 2021, as at October 2021). The country’s first three waves had roughly tracked those of South Africa, where 2–5 million Zimbabweans are estimated to live, and between which there is significant traffic, both legal and illegal. Current control measures were among the more stringent of the study countries, with many vaccine mandates in place (discussed in Section 4.1.2).
Zimbabwe has stronger international relations with China than with Western governments and geopolitics has clearly contributed to the choice of Covid-19 vaccine. As our study took place, the country had purchased around 12 million doses of Chinese-made vaccines, with more planned (Kyobutungi 2021), and our survey respondents reported Sinovac and Sinopharm as the main types available in their communities. COVAX had recently delivered its first consignment to Zimbabwe of 1 million doses of Sinopharm, stating that ‘for consistency’ it would continue to be the main vaccine Zimbabwe received through the programme (COVAX 2021). Barring a few distribution hitches, vaccines continue to be available, with ongoing government campaigns to encourage uptake.
We surveyed male and female youth leaders, federation leaders, religious leaders, and community health-care workers from five informal/slum settlements across Harare, including some in peri‑urban areas (Figure 2). Three-quarters of respondents are self-employed and 10 per cent are casually employed. On average, 90 per cent said that the pandemic had negatively affected their income.
Many factors are contributing to the pandemic’s impact on jobs and livelihoods in informal settlements in Harare. Informal dwellers’ incomes have been particularly affected, directly and indirectly, as business slowed and companies retrenched. Wholesale farmers’ markets were closed, cutting off vendors’ access to fruit, grain, and vegetables for resale. Market stall demolitions left many self-employed people jobless. Stringent lockdown measures restricted movement even within the city, cutting off workers from workplaces, and vendors were not classified as essential services providers and so could not get travel permits.
Official government Covid-19 vaccine rollout available to communities had begun in the survey areas between February and July 2021. National and province vaccine statistics are shared daily by the government, but there are no government sources providing city-level information, let alone a settlement or local centre. In terms of take up, there was little agreement among the few community leaders willing to estimate the scale of vaccine uptake in their settlements in the two weeks immediately prior to the survey – for example, Hopley settlement estimates ranged from 300–2,500 people.
In four of the five areas, vaccination was taking place in or near to the settlement, albeit with discouragingly long queues at many centres. Vaccination centres were ordinarily set up in existing health facilities and so in Stoneridge, where there is no health centre, residents had to travel outside the local area. In some of the other settlements, leaders knew no one who had gone elsewhere; while in others, people were travelling further to find shorter queues or being vaccinated in workplaces as government employees (e.g. civil servants, health workers, soldiers).
At the time the survey took place, all adults were eligible for free vaccination. However, the long queues come with costs – time away from jobs or businesses and infection risks in crowded health centres, or walking time or bus fare to travel to centres where queues are shorter. For those who can afford it, private health facilities had recently been permitted to offer vaccination for a fee (under US$5), which was expected to reduce queues in government centres. However, there was little awareness of this option among the community leaders, unsurprising since the study settlements are predominantly served by government health-care facilities.
We asked respondents to reflect on gendered dimensions of vaccine uptake in their communities. A third of community leaders saw little difference in uptake between men and women, while others related observed differences in men’s and women’s motivations regarding vaccine mandates aimed at particular segments of the local economy. Men were more likely to be formally employed and required by employers to be vaccinated. Women spend more time both trading and shopping in informal markets, where vaccination was also required for traders.
Vaccination in Zimbabwe was officially voluntary, but the growing number of mandates meant that this is not necessarily how it has been experienced on the ground. Vaccines were required for state employees, for those visiting government offices and travelling on buses, for market traders, and many other areas of life. Nevertheless, the reported long queues suggested demand still exceeding supply, thereby constraining people who would have liked to be vaccinated but could not from participating in social and economic life (Matimaire 2021). At the time of writing, the country’s biggest trade union was taking to court both the government and private companies, challenging mandatory employee vaccination (Chingono 2021).
We found differences across Harare settlements in the availability of public health information about Covid-19 vaccines and vaccinations. In many areas, people’s only information sources were nationwide Ministry of Health campaigns on social media, radio, and television, with little local information disseminated. A few communities received locally specific information via non‑governmental organisation (NGO)-led awareness campaigns, community health workers, and nearby clinics.
Hesitancy appeared generally low but concentrated in particular groups. Early in the pandemic, informal settlement residents in Harare reported that, although misinformation and conspiracy theories were being pushed on social media, in general, people are not convinced by them and most want access to vaccines for the end of the health and economic emergency (Mitlin et al. 2020). We found this to still be the case. Of the four study cities, Harare community leaders were the most positive about Covid-19 vaccines. They knew people who had died and wanted to protect their own health, feel safe in public, and attend their churches, which had vaccine mandates. In their communities, hesitancy was more significantly present: 16 per cent of respondents knew someone who had recently refused a vaccine, many of whom belonged to Apostolic faith groups where attitudes to vaccines are often negative.9 However, our Harare researchers also observed an encouraging number of Apostolic church leaders promoting vaccination to their congregants.
At the end of September 2021, 4 per cent (820,000) of Malawi’s population had received at least one Covid-19 vaccination, with 2.5 per cent (500,000) fully vaccinated; cumulative reported cases were 61,580 (3,134 per million) and official deaths 2,282 (Our World in Data n.d., as at 30 September 2021). Excess death estimates in October 2021 set Malawi’s real figure at between 2,400 and 36,000 people – an indication of the size of the data gap. Barring the early weeks of the pandemic, lockdown measures had been relatively few and community leaders reported that restrictions were only loosely enforced or observed. Vaccine mandates were not widespread, although some unvaccinated government workers were required to work from home and a small number of private companies were incentivising their employees to be vaccinated.
Malawi is a low-income country that relies on COVAX and largely Western donors for Covid-19 vaccines. At the time our study took place, Malawi’s vaccine rollout had been repeatedly challenged by issues of low and inconsistent supply – having at that point received only 1.6 million doses, mostly through COVAX, and in nine different consignments from at least six different countries. Figure 3 compares Malawi’s fluctuating supply with vaccination rates (Our World in Data n.d., as at 30 September 2021; Kyobutungi 2021).
We spoke to community leaders from five inner-city informal settlements in Lilongwe (Figure 4). They were male and female traditional leaders, youth leaders, community health-care workers, federation leaders, and religious leaders, aged 22–63 years. Sixty per cent were self-employed, 22 per cent casually employed, and 13 per cent formally employed. On average, 87 per cent said their own income had been negatively affected by and during the pandemic.
Informal settlement communities in Lilongwe are focused on recovering from economic shock and we found that, for many people, getting a Covid-19 vaccine was simply not a priority. Although Malawi itself had imposed relatively few lockdown restrictions, international travel restrictions compounded by the global economic crisis have hit hard. Self-employed people in the survey areas have lost businesses and capital due to price rises and associated lack of supply of many everyday commodities (for example, cooking oil) which are imported from countries such as South Africa and China to be resold in informal settlements. Impacts are citywide, because many residents of wealthier areas also depend on Lilongwe’s informal markets. In settlements near industrial areas, retrenchments have affected casual labourers and vendors catering to workers. And in the general economic downturn, people living in settlements situated near wealthy residential areas have lost jobs as domestic workers and security guards.
Covid-19 vaccination began to be rolled out in the survey areas between March and July 2021. As the survey took place, vaccination was free and universally available. There appeared to be no alternatives to government rollout, legal or illegal, although vaccination certificates could reportedly be obtained for a bribe. There was little certainty about the scale of vaccine uptake. Of the few community leaders willing to give estimates, numbers were low and wide-ranging – between 4 and 70 people in an area in the two weeks immediately preceding the survey.
Of the four cities, Lilongwe communities were least able to access vaccines close to where they lived. Two settlements, Chinsapo and Mtandire, are near to vaccinating hospitals, but residents of others must walk or travel to public health centres at discouragingly long distances. Despite this, but in line with overall low vaccination rates, only four respondents knew of anyone who had got a vaccine outside of their local area – male government employees at their workplace, and women neighbours who had travelled further away because their local centre had run out of doses.
When asked about gender differences in vaccine uptake in their settlement, community leaders’ responses varied. Women were perceived to be more easily put off by misinformation, but also more comfortable following official health advice. Men are more likely to be formally employed and subject to employee vaccination requirements but have less (or less flexible) time than women to queue at health centres. A Lilongwe community leader stated, ‘Women are so used to other injections during pregnancy or family planning… so this vaccine is not anything new’.
Superficially, vaccine hesitancy in Lilongwe communities appears widespread, fuelled by misinformation. The community leaders reported a culture of secrecy, where many who do get vaccinated do not advertise their decision to friends and neighbours. Many respondents personally knew someone who had refused a Covid-19 vaccine, for example because they believed messages from church leaders that the vaccine led to devil worship. Several community leaders themselves expressed concern about health and fertility risks, and others did not feel it was a priority.
However, the vast majority of community leaders (83 per cent) were positive about Covid-19 vaccines – they dismissed the conspiracy theories, many had already been vaccinated, and they were working to keep the issue live in federation discussions during routine activities such as savings group monitoring and settlement profiling exercises. One Lilongwe community member shared, ‘Two of my friends were open enough to say that they went for vaccination. Most people are going for vaccination in secret because of the conspiracy theories and at the same time, they want to be protected’.
New vaccine types can reignite public fears about safety. In Malawi, initial uptake was low when the vaccine rollout launched with AstraZeneca vaccines, and in May 2021 the government destroyed 20,000 recently expired doses, hoping to increase public confidence (Figure 3). Uptake improved, then declined again in August after the country’s first Johnson & Johnson consignment, as people again chose to wait for evidence of the new vaccine’s safety.
We found information disseminated in Lilongwe communities about Covid-19 vaccines and vaccinations varied by settlement. As in Harare, respondents reported a dearth of practical and locally specific official information. The only vaccination statistics publicly shared are at country level by the national government. Locally specific reports – for example, numbers vaccinated daily at a particular health centre – could provide evidence and reassurance to hesitant communities that many people in their area are getting vaccinated without adverse consequences. Practical information was also reported to be lacking, for example about different vaccine types, where to go, and availability at local centres.
As our study began, Uganda had the lowest vaccination rate among the study countries: 3.5 per cent of the population had received at least one dose (1.64 million people) and under 1 per cent were fully vaccinated (416,000) (Our World in Data n.d., as at 30 September 2021). Official cumulative figures at this time were 123,572 cases (2,622 per million population) and 3,152 deaths (67 per million population), with a wide estimate of excess deaths between 2,300 and 68,000 (The Economist, as at October 2021). A second wave in June 2021 led to a countrywide lockdown for over a month, and a curfew remained in Kampala throughout the study period. Public transport was operating at restricted capacity and people were required to wear masks and observe social distancing, although observance and enforcement were reportedly low.
As of September 2021, Uganda had received a total of 1.8 million doses, in eight consignments consisting of four different vaccine types, and from at least six different countries (direct donations or through COVAX). When our study started, vaccines were publicly administered, with the country reportedly considering options for private channels, and Uganda was the only study country yet to announce universal eligibility for adults (this happened in late January 2022). People due a second dose and high-risk groups continued to be prioritised (health-care workers, security personnel, over-50s, teachers, those with underlying health conditions). Community leaders also reported vaccine mandates in place in Kampala for teachers, some market vendors, and hospital staff.
We spoke to community leaders from informal areas in each of Kampala’s five divisions (Figure 5): male and female traditional leaders, youth leaders, federation leaders, religious leaders, and (nearly one-third) community health volunteers; aged between 18 and 69 years. On average, 90 per cent said that their income had been affected negatively by and during the pandemic. Sixty‑two per cent are self-employed, 23 per cent casually employed, and 9 per cent formally employed.
A relatively high proportion of respondents (25 per cent) said that no official vaccine rollout was taking place in their city. Most others said it had only just started, in August or September 2021. In four of the five survey areas, vaccination was happening in or near to settlements, in churches, hospitals, health centres, and municipal offices. The communities who lived in Kampala Central Division had to travel outside their local area to be vaccinated.
There was little knowledge of local levels of uptake. Among the few leaders willing to estimate the number of people from their settlement who had been vaccinated in the two weeks immediately preceding the survey, uptake was thought to be low: between 6 and 100 people in a settlement. Many noticed no gender differences in uptake in their community, while some observed that men were more likely to be subject to employment-related vaccine mandates, for example as market vendors, government workers, and truck drivers, or as motorcycle taxi drivers who want to enter areas requiring vaccine certificates. Women were also seen to be motivated for livelihood-related reasons and because they take the health risks to themselves and their families more seriously.
Kampala community leaders were vocal that they wanted lockdown measures to end. The pandemic has hit livelihoods hard, and vaccination rollout is understood as one path towards reopening the economy. Most said that if a Covid-19 vaccine was made immediately available to them, they would definitely get it10 and several respondents also talked about their responsibility as leaders to set an example in their community. At the same time, hesitancy and the effects of misinformation were clearly present among some survey respondents, as well as reportedly being pervasive in their communities, with concerns around safety and side effects of particular vaccine types, and a general lack of faith in government.
I was eligible… I was told that if I get vaccinated, I cannot die of Covid-19. I had fear and I was told that in case you have some complications in the body, it’s not good to get vaccinated.
(Community leader, Rubaga Division, Kampala)
Most respondents said some information was being disseminated in their communities, mostly national and local government encouraging them to protect their health and the health of their families. Radio, television, and local NGOs were the main sources. Many of the leaders had themselves been involved in the vaccine rollout in their communities – for example, in vaccine administration, sensitisation, and information-sharing (including touring settlements with megaphones informing people about vaccine availability at nearby centres), door-to-door visits with government-sponsored ‘village health teams’, and as SDI federation task forces trained in handling Covid-19 health emergencies in their communities.
When our study took place, India had vaccinated 47 per cent of its population with at least one dose, with 17 per cent fully vaccinated (Our World in Data n.d., as at 30 September 2021). Much of the unvaccinated population also have Covid-19 antibodies, having been exposed to the virus during the huge second wave that began in March 2021 (Dasgupta 2021). Cumulative official figures were 33.8 million cases (24,233 per million population) and 448,000 deaths (322 per million), with much higher excess death estimates, between 1.1 million and 6.9 million (The Economist 2021, as at October 2021).
India was the only study country manufacturing Covid-19 vaccines, making the picture of access very different. The April 2021 export ban drastically diminished supplies elsewhere, notably for the COVAX programme, but allowed the country to speed up administration to over 5 million doses a day (Our World in Data n.d.). Supply and distribution issues nevertheless persist, and the situation has varied widely across states and cities. Dimensions of inequity characterising India’s Covid-19 vaccination rollout have included: (1) to rural and remote locations; (2) people lacking access to the technology needed to navigate the online registration system; and (3) a gender gap which has emerged with more men than women being vaccinated.
During the study, vaccines were also available privately and at a (capped) cost. Indian manufacturers could sell 10 per cent of their doses on the Indian private market and the remaining 90 per cent at a far lower price to the federal government, which then made allocations to states. If, for example, federal allocations did not meet public demand, states could also purchase on the private market – in competition with private hospitals, for instance, which pass on costs to patients.
Adequate local-level data was not available for the three African cities; however, it is possible to provide some city-level context for Mumbai. As our study began, the city’s vaccination rates were among India’s highest: 90 per cent of the adult population had received one vaccination, with around half fully vaccinated (Debroy 2021). By October 2021, 13.6 million doses had been administered through both public and private channels, at an average of about 49,000 per day (MCGM 2021a).
Including Mumbai in our study allows us to examine a successful vaccine rollout in a context with a large number of informal settlements. However, it is in many ways a very different case – not least in the scale of vaccine challenge, having a core city population about the size of Zimbabwe, set within a wider municipal area, and with commuter transport links to large peripheral metropolitan regions.
In terms of how people access vaccines, although routine vaccines are conducted under India’s health system, Covid-19 vaccination in Mumbai is a political event delivered through structures and budgets controlled by elected representatives and taking place in specialist centres often advertising the name and face of the local political leader who facilitated their establishment. This has given much energy to the process and led to the establishment of a large number of vaccination centres: by September 2021, Mumbai municipality had 322 free, state‑run centres (MCGM 2021b) and 95 private hospitals vaccinating for a cost of INR 780 (about US$10) (Pinto 2021). Smaller centres dispense around 200 doses each day and larger ones around 2,000 a day.
Political power in Mumbai is very grass roots and half of the city lives in informal settlements, so representation and voice of low-income communities is correspondingly greater. There have therefore been efforts to make Covid-19 vaccine delivery fairer, not least for political reasons. Examples include reducing the proportion of vaccination appointments that could only be made online, or only allowing in-person booking or walk-ins at centres within informal settlements often – although the latter has also led to problems. In one instance, where infection risk was being increased by heavy demand resulting in crowds around a vaccination centre, local women set up a registration desk where people could leave phone numbers on a first-registered-first-served basis. Local SDI federation groups have also been involved in facilitating online registration for those in their communities who need help using technology.
Many Indian politicians understand that vaccinating informal workers is a key step towards economic recovery. Nationally, the informal sector comprises 90 per cent of India’s labour force (in urban areas the proportion is 80 per cent) (Raveendran and Vanek 2020). It has been hit hard by and during the pandemic and impacts of earlier restrictions continue to be felt: many migrant workers left cities for rural areas and have not returned, leading to a fall in the remittances upon which much of India’s rural economy depends. Politicians have urged private companies to help finance the vaccination drive, for example by covering the costs of low-income people to be vaccinated at private hospitals, and amendments to laws governing corporate social responsibility obligations allow vaccine rollout to also be funded through this channel. An emerging trend in Mumbai is for charitable donors and philanthropists to purchase private market vaccines and donate them to local government or NGOs, for free or discounted public administration.
Very early in the pandemic, travel on local trains was restricted to essential workers. Subsequent state government decisions to impose a vaccine mandate on public transport were therefore big drivers of vaccine uptake, finally allowing a fully vaccinated general public to travel again. This has led many to lobby their local political representatives to improve vaccine access by, for example, establishing a local centre. Other control measures during the study period including face masks in public, but our survey respondents reported no lockdowns or curfews.
We spoke to male and female community leaders from six informal settlements or slum resettlement colonies in Mumbai municipality (Figure 6), including traditional leaders, youth leaders, federation leaders, community health-care workers, women’s group leaders, and area society leaders; aged between 25 and 67. Twenty-nine per cent were self-employed, 36 per cent casually employed, and 10 per cent formally employed. On average, 76 per cent said their income had been negatively affected during the pandemic, the lowest of the study cities, although this varied considerably by settlement; overall, 22 per cent said their income had not been affected.
Covid-19 vaccine rollout had begun in most areas between April and July 2021. All adults were eligible and Covishield was the type most available to communities. Vaccines were available in or near most settlements, although many respondents flagged low supplies and long queues. Venues included public and private hospitals, health centres, schools, and community halls. Only a few respondents from Relocation Colonies and M. East Ward reported that vaccines were not available in their local area. Overall, 20 per cent of Mumbai community leaders knew someone who had received a vaccine outside of the local area, either at work or forced to travel because of overcrowding and long queues at closer centres. Many Mumbai employers offer to pay for employees and employees’ immediate family to be vaccinated at private centres, including in informal employments such as domestic work, drivers, and carers. Many respondents knew people who had paid for vaccination at private hospitals, and they are likely referring to these kinds of cases.
Informal settlements in Mumbai are large, and those chosen for the survey have a minimum of 5,000 households each. Airport settlement is estimated at 80,000 households and Dharavi, one of Asia’s largest slums, has a population of nearly 1 million. Most respondents could estimate roughly how many people in their local area had recently received a Covid-19 vaccine and more than half of those who did said that over 2,500 people (in one case, 8,000) had been vaccinated in their local area in the two weeks immediately preceding the survey.
Respondents observed few gendered differences in uptake in their communities, despite that, overall during the study, women made up 42 per cent of those vaccinated in Mumbai (Indian Ministry of Health and Family Welfare 2021). Official city statistics present a dynamic picture of Mumbai vaccination by age, gender, and social segment, but local breakdowns are not publicly available. During the study, specific days were being reserved for vaccinating women, teachers, and students aged over 18, frequently timed to the reopening of educational institutions.
Survey results revealed little hesitancy. Community leaders were overwhelmingly positive about Covid-19 vaccination, and few knew of anyone in their communities who had recently refused a Covid-19 vaccine. Early in the city’s vaccine rollout timeline, misinformation had circulated widely, with hesitancy even among initially eligible essential workers. However, uptake improved after the vaccination was made available to all adults in May 2021, and many of the earlier rumours melted away. Our researchers found that the little hesitancy still remaining in communities largely related to adverse side effects, but most people were eager to get vaccinated.
Vaccine availability constrains the room for good policy decisions
The cities in our study exemplify, in different ways, that vaccine availability constrains the room countries have to make good policy decisions about low-income communities. In Mumbai, India’s vaccine manufacturing status guarantees a steady supply, giving local politicians confidence to invest their own reputations in administering the rollout. In Lilongwe and Kampala, as our study took place, political will was likely undermined by low and unreliable supply due to patent restrictions and geopolitical issues. However, in the weeks following our study, Uganda’s situation changed dramatically. The government took delivery in mid-September 2021 of 2.5 million doses of a fifth vaccine type (Johnson & Johnson) and announced that a further 18 million doses of China’s Sinopharm were expected in phases from October 2021. The subsequent rollout shows what a sufficient and reliable supply might achieve, with Uganda’s vaccination rate increasing over the next four months from 3.5 per cent to 29 per cent (share of population receiving one dose; Our World in Data n.d., as at 9 March 2022), overtaking Zimbabwe in February 2022.
Wider geopolitical alliances are also part of the vaccine supply picture and likely influence countries’ future capacity to manage the Covid-19 virus as the pandemic continues to develop. In the case of Uganda, it perhaps cements the established turn of much of sub-Saharan Africa towards relationships with China. In the case of Zimbabwe, the government has stronger international relations with the Chinese government than with Western governments and has had long-standing and relatively reliable access to Chinese-made vaccines since quite early in the global rollout.
The effects on vulnerable communities of restrictions based on vaccination status
In Mumbai, with good vaccine supply and a relatively strong political voice for low-income communities, vaccine mandates have given some democratic impetus to the rollout. Residents, keen to use public transport again, lobbied local politicians, resulting in the establishment of huge numbers of local vaccination centres including in informal settlements. However, communities may be subject to restrictions based on vaccination status even when they face challenges accessing vaccines. In Lilongwe, where low national supply limited local availability, only a few company or government employees were reported to be subject to such restrictions. In Kampala, vaccine mandates for some groups including teachers and hospital workers were in place at the time of our study, despite very limited access. And in Harare, where communities were subject to many mandates, local distributional challenges put a high cost on getting a vaccine for some people. As our study took place, rollout in Harare was mostly through existing public health-care providers and survey respondents’ reports of queues at local clinics and people travelling long distances indicate that these were not always meeting demand. In Zimbabwe, there has been some pushback against state management and mandates; for example, the trade union actions mentioned above.
Harare has imposed vaccination mandates on informal sector activities, including informal traders, raising questions of what this might mean for relationships between authorities and informal operators in other or general contexts if such practices become more widespread.
Gender implications in vaccine access and uptake are important
Where disaggregated data is available, gender differences in vaccine uptake are observed differently in several contexts. Differences include relating to challenges in accessing vaccines and in experiences of Covid-19 health risks and vaccine mandates or restrictions. In South Africa, official statistics showed that many more women than men are getting vaccinated; suggested explanations include that women tend to dominate professions with high infection risks (such as health care, teaching, and informal street traders) and men are more put off by long queues (Gibbs 2021). In contrast, India’s data showed more men getting vaccinated, as traditionally patriarchal households prioritised vaccination for men and because women have poorer access to the technology and information needed to register for a Covid-19 vaccine or are unable to go to centres alone especially where these are not nearby (Guha 2021).
Our respondents’ perspectives on gender dimensions to uptake were interesting. Broadly, at least in the African cities, it seems that women tend to be more willing and more comfortable with health-care systems, and that men, who are more often in formal employment, are more likely to be subject to both mandates and opportunities to be vaccinated at work. Mumbai respondents observed few differences.
Information is lacking about who is being vaccinated in communities and cities
In general, people had little sense of who and how many were vaccinated in their communities. In Mumbai, knowledge was better: local-level statistics are more readily available and the process for distributing vaccines to centres is more transparent. In the three African cities, during our study period at least, little city information was available, let alone more granular information. For instance, in Lilongwe, broader vaccine supply issues appeared to be compounded by challenges of public hesitancy, misinformation, and a lack of trusted, practical, and locally specific information about the vaccination rollout. Accessible information from sources that communities listen to is perhaps especially crucial to encourage vaccination uptake in contexts such as Lilongwe, where communities are generally subject to few vaccine mandates, where the health risks are perceived to be low, and where many people do not prioritise getting vaccinated as a route towards economic recovery.
Allowing communities to begin to see evidence of local uptake with their own eyes by making local-level statistics about vaccine uptake available (for example, the past week’s numbers posted at health centres or information disseminated through local groups or radio stations) might help tackle hesitancy and dissolve circulating myths more effectively than national statements tweeted by the Ministry of Health.
Hesitancy
Public Covid-19 vaccine hesitancy is clearly not just a barrier to uptake in rich countries, and it is important that research on the harm misinformation causes looks at how it is spreading differently around the world. Misinformation appeared widespread in many of the study areas, particularly in Lilongwe and Kampala. Some people had religious reasons, some had safety concerns fuelled by real medical uncertainty, or lack of access to reliable and culturally useful sources of information. Others just did not see it as a priority in light of their other struggles, exacerbated by the pandemic. Our survey also revealed many people who would like to have a jab that cannot get one, a situation Mumbai has managed to overcome.
The community leaders are highly attuned to the nuances of motivation and hesitancy in their communities. Some were actively conducting awareness drives, sharing information, and busting myths door-to-door or at community gatherings. Several were motivated to get vaccinated in order to set an example. They also understand the kinds of barriers communities face when they do want to get vaccines: long queues; unfamiliar, inadequate, or corrupt health systems; travel costs or walking time; lost earnings being away from work; and lack of reliable information about when and where vaccines are available near them.
The examples from Mumbai also show how local leaders and organised community groups are playing crucial roles in facilitating the vaccine rollout in their areas. They understand the practical arrangements necessary to make sure that people can access vaccines when they are on offer and are an important source of local knowledge upon which governments can draw to improve uptake in informal and low-income urban areas, to ensure that rollout is equitable, and that those hardest hit by the pandemic are protected first.
Mumbai’s success, in terms of scale of effort and number of centres – many strategically placed close to informal settlements or relocation colonies – was driven by a combination of reliable supply and high levels of willingness from political leaders, making the connection between vaccination, economic recovery, and protecting the informal sector from further lockdowns. Some of the other national contexts in which our study took place often had a limited or inconsistent vaccine supply, in the face of overwhelming demand for the first or subsequent specific jabs. One question is how public attitudes will change if and when vaccine rollouts gain momentum and people’s chances improve of actually being able to receive a Covid-19 vaccine if they want one.
Final thoughts
The voices coming from our survey are clear that informal settlement communities have been hit hard and badly want the pandemic to be over. On average and across the four cities in our study, over half of respondents said that ‘nearly all’ or ‘most’ people in their informal settlement who usually worked informally were no longer working; and a quarter said that ‘nearly all’ or ‘most’ of those in formal employment had been laid off. Speaking of themselves, 85 per cent said that their own incomes had been negatively affected – rising to 88 per cent of women, 95 per cent of self-employed respondents, and 94 per cent of community health workers. Of those who belong to a savings group, 90 per cent said that their savings and those of their group had been negatively affected.11
The leaders we spoke to understand access to vaccines as one measure among many needed towards their communities’ health, social, and economic recovery. Among others, the pandemic has highlighted the importance of mutual support networks, such as savings groups, as critical grass-roots safety nets that cushion the urban poor in times of shocks. Throughout, federations across the global SDI network have worked to address basic sanitation needs, collect data to tailor responses, strengthen safety nets through networks of women-led savings groups, and raise awareness online and in neighbourhoods – demonstrating the central role that organised communities can play in responding to crises and ensuring local humanitarian efforts reach those in need (Cities Alliance 2021). But this is in the absence of access to social protection (although in Peru, South Africa, and more recently Kenya, some efforts appear to have been made, e.g. Alfers et al. 2020). Governments and humanitarian relief efforts must draw on local knowledge to understand and support communities in their efforts to recover and rebuild resilience and must work to resolve the underlying inequities that led to this disproportionate devastation through, for example, provision of adequate basic services, health care, and tenure security.
* This IDS Bulletin was funded by the UK government’s Foreign, Commonwealth & Development Office (FCDO) through the Covid Collective. The Collective brings together the expertise of UK- and Southern-based research partner organisations and offers a rapid social science research response to inform decision-making on some of the most pressing Covid-19-related development challenges. The Covid Collective cannot be held responsible for errors, omissions, or any consequences arising from the use of information contained. Any views and opinions expressed do not necessarily reflect those of FCDO, the Covid Collective, or any other contributing organisation. For further information, please contact: covid-collective.net.
† Our thanks to the city-based researchers in Harare, Kampala, Lilongwe, and Mumbai who were involved in the study. In Harare (all Dialogue on Shelter), these were George Masimba (research coordinator), Thomas Karakadzai, Anna Teurai Nyamangara, Sheila Muganyi, Rudo Chikumbindi, and Artwell Nyirenda. In Kampala, these included Loubega Edris, and in Mumbai, Sharmila Gimonkar, among others. We are grateful to the 300+ community leaders who were our respondents for some or all of the six survey rounds, for their patience and willingness to share their knowledge and answer our questions every fortnight. Lastly, our thanks to the leaders and members of national federations of the urban poor in each city, for linking the research teams to the interviewees. In Harare: Zimbabwe Homeless People’s Federation. In Kampala: National Slum Dwellers Federation of Uganda (NSDFU). In Lilongwe: Malawian Federation of the Rural and Urban Poor. In Mumbai: Mahila Milan and the Indian National Slum Dwellers Federation (NSDF). Thanks also to Beth Chitikwe-Biti at Shack/Slum Dwellers International (SDI) for steering in the design stages.
‡ This study was funded by the UK Foreign, Commonwealth & Development Office (FCDO) as part of the University of Manchester’s involvement in the Covid Collective research platform.
1 Kate Lines, research consultant and Honorary Research Fellow, Global Development Institute, University of Manchester, UK.
2 Junior Alves Sebbanja, Project Manager, ACTogether Uganda, Uganda.
3 Stanley Dzimadzi, Community Data for Change Officer, Centre for Community Organization and Development (CCODE) Malawi, Malawi.
4 Diana Mitlin, Professor of Global Urbanism, Global Development Institute, University of Manchester, UK.
5 Patience Mudimu-Matsangaise, Director, Dialogue on Shelter for the Homeless Trust, Zimbabwe.
6 Vinodkumar Rao, Programme Manager, Society for the Promotion of Area Resource Centres (SPARC), India.
7 Happiness Zidana, Learning, Compliance and Quality Assurance Officer, CCODE Malawi, Malawi.
8 Most other African countries to have met this goal have relatively small populations and many are small island developing states.
9 As much as 37 per cent of Zimbabwe’s population belongs to Apostolic communities (US Embassy in Zimbabwe 2020).
10 Based on a question asked in a multi-country survey by Imperial College London and YouGov; see YouGov Covid 19 Behaviour Tracker Data Hub.
11 Figures are average responses across cities and surveys. The relevant questions were asked twice, once in mid-August and once in late November 2021. As expected, responses relating to the pandemic’s overall impact on respondents’ own incomes and savings showed little change between August to November, while responses relating to the current status of informal and formal workers in the surveyed communities indicated that employment prospects for both groups improved somewhat over the interval, although with variation and some counter trends at city and settlement levels. A full report on the study’s data findings will be published later in 2022 on the Covid Collective website.
Africa CDC (2021) COVID-19 Vaccine Perceptions: A 15 Country Study, Centres for Disease Control and Prevention (accessed 27 May 2022)
Alfers, L.; Ismail, G. and Valdivia, M. (2020) Informal Workers and the Social Protection Response to COVID-19: Who got Relief? How? And Did It Make a Difference?, WIEGO Policy Insights 2, Manchester: Women in Informal Employment: Globalizing and Organizing (accessed 9 March 2022)
Badiuzzaman, M. and Akter, N. (2021) Covid-19 Vaccination and Digital Exclusion at the Margins, Covid Collective blog, 13 July (accessed 9 March 2022)
Brackstone, K. et al. (2021) ‘Examining Determinants of COVID-19 Vaccine Hesitancy in Togo’, Figshare Policy Brief, DOI: 10.6084/m9.figshare.14805765.v1 (accessed 13 May 2022)
Braham, C. and Ogando, A.C. (2021) Essential, but Unprotected: How Have Informal Workers Navigated the Health Risks of the Pandemic?, WIEGO Policy Insights 4, Manchester: Women in Informal Employment: Globalizing and Organizing (accessed 9 March 2022)
Chingono, N. (2021) ‘ “No One May Be Compelled”: Zimbabwe Unions go to Court over Covid Jabs’, The Guardian, 7 September (accessed 9 March 2022)
Cities Alliance (2021) Predicting Covid-19 Contagion Risk Hotspots, 16 March (accessed 9 March 2022)
Corburn, J. et al. (2021) ‘Correction to: Slum Health: Arresting COVID-19 and Improving Well-Being in Urban Informal Settlements’, Journal of Urban Health 98: 309–10, DOI: 10.1007/s11524-020-00491-1 (accessed 13 May 2022)
COVAX (2021) IAVG Vaccine Allocation Decision for Round 7, 17 September (accessed 9 March 2022)
Dasgupta, R. (2021) ‘After India’s Brutal Coronavirus Wave, Two‑Thirds of Population has been Exposed to SARS-CoV2’, The Conversation, 20 August (accessed 9 March 2022)
Debroy, S. (2021) ‘50% Mumbai’s Adult Population Fully Vaccinated, 93% Given 1st Jab’, The Times of India, 7 October (accessed 9 March 2022)
Dupraz-Dobias, P. (2020) ‘COVID-19 Shifts Peru’s Internal Migration into Reverse’, The New Humanitarian, 8 July (accessed 9 March 2022)
Economist Intelligence Unit (2021) How Much Will Vaccine Inequity Cost?, London: Economist Intelligence Unit
Gibbs, A. (2021) ‘Men are Slower to get COVID-19 Vaccines in South Africa: Lessons from HIV Research’, The Conversation, 2 September (accessed 9 March 2022)
Guha, N. (2021) ‘India’s Covid Gender Gap: Women Left Behind in Vaccination Drive’, The Guardian, 28 June (accessed 9 March 2022)
Horner, R. (2021) ‘Covax Misses its 2021 Delivery Target – What’s Gone Wrong in the Fight Against Vaccine Nationalism?’, The Conversation, 17 September (accessed 9 March 2022)
ILO (2021) ‘An Update on the Youth Labour Market Impact of the COVID-19 Crisis’, Statistical Brief, Geneva: International Labour Organization (accessed 9 March 2022)
IMF (2021) World Economic Outlook, Washington DC: International Monetary Fund
Indian Ministry of Health and Family Welfare (2021) CoWIN Dashboard (accessed 13 May 2022)
Jerving, S. (2021) ‘COVID-19 Vaccine Alliance Chair: African Political Leadership Lacking’, Devex, 16 September (accessed 9 March 2022)
Kyobutungi, C. (2021) ‘Want to Know about Vaccine Rollouts in Africa? Click on a Country Here and Find Out’, The Conversation, 28 September (accessed 9 March 2022)
Lenhardt, A. (2021) The Social Economic Impact of Covid-19 in Informal Urban Settlements, Covid Collective Helpdesk Report 8, Brighton: Institute of Development Studies, DOI: 10.19088/CC.2021.008 (accessed 13 May 2022)
Matimaire, K. (2021) ‘Informal Traders Appeal for Onsite Vaccination’, New Zimbabwe, 7 August (accessed 9 March 2022)
MCGM (2021a) BMC Covid-19 Response War Room Dashboard (accessed 20 October 2021)
MCGM (2021b) List of Active Public COVID Vaccination Centres in Mumbai (as on 07.09.2021), Municipal Corporation of Greater Mumbai (accessed 9 March 2022)
Mitlin, D.; Haddis, F.; Makau, J.; Nyama, G.M. and Molokoane, R. (2020) Vaccines, Information and the Ongoing Crisis of Affordability for the Urban Poor, IDS Opinion, blog, 18 December (accessed 9 March 2022)
Our World in Data (n.d.) Coronavirus (COVID-19) Vaccinations (accessed 9 March 2022)
Pinto, R. (2021) ‘Amid Several Vaccination Scams, BMC Releases List of Private Vaccine Centres’, Times of India, 2 July (accessed 9 March 2022)
Raveendran, G. and Vanek, J. (2020) ‘Informal Workers in India: A Statistical Profile’, WIEGO Statistical Brief 24, Manchester: Women in Informal Employment: Globalizing and Organizing (accessed 9 March 2022)
Sánchez-Páramo, C. (2020) The New Poor Are Different: Who They Are and Why It Matters, World Bank blogs, 13 August (accessed 9 March 2022)
Schiffling, S. (2021) ‘COVID Vaccines: How to Speed up Rollout in Poorer Countries’, The Conversation, 5 October (accessed 13 May 2022)
Shupler, M. et al. (2021) ‘COVID-19 Impacts on Household Energy and Food Security in a Kenyan Informal Settlement: The Need for Integrated Approaches to the SDGs’, Renewable and Sustainable Energy Reviews 144: 111018, DOI: 10.1016/j.rser.2021.111018 (accessed 13 May 2022)
The Economist (2021) ‘The Pandemic’s True Death Toll’, 2 November (accessed 11 March 2022)
UNDP (n.d.) Global Dashboard for Vaccine Equity (accessed 9 March 2022)
United Nations Malawi (2021) Malawi COVID Situation Update No.43 – 6 August 2021 (accessed 27 May 2022)
US Embassy in Zimbabwe (2020) Zimbabwe 2020 International Religious Freedom Report (accessed 27 May 2022)
WHO (2020) SAGE Values Framework for the Allocation and Prioritization of COVID-19 Vaccination, Geneva: World Health Organization
World Bank (2022) Country and Lending Groups, World Bank Data (accessed 27 May 2022)
World Bank (2020) GDP Data, World Bank Databank (accessed 27 May 2022)
© 2022 The Authors. IDS Bulletin © Institute of Development Studies. © Crown Copyright 2022. | DOI: 10.19088/1968-2022.128
This is an Open Access article distributed for non-commercial purposes under the terms of the Open Government Licence 3.0, which permits use, copying, publication, distribution and adaptation, provided the original authors and source are credited and the work is not used for commercial purposes.
The IDS Bulletin is published by Institute of Development Studies, Library Road, Brighton BN1 9RE, UK This article is part of IDS Bulletin Vol. 53 No. 3 July 2022 ‘Pandemic Perspectives: Why Different Voices and Views Matter’; the Introduction is also recommended reading.
{kind=link}